
Governors decry UAW push to unionize car factories in southern states
Republican governors criticized the UAW's efforts as Volkswagen workers in Tennessee are set to start voting on joining the labor union.
Watch CBS News
Republican governors criticized the UAW's efforts as Volkswagen workers in Tennessee are set to start voting on joining the labor union.

The former president's media company announced plans to air news, religious channels and other content.

The union for American Airlines pilots says it's been seeing "a significant spike in safety- and maintenance-related problems in our operation."

19 people have been stricken — including nine who have been hospitalized — after getting fake or mishandled injections in homes and spas, feds warn.
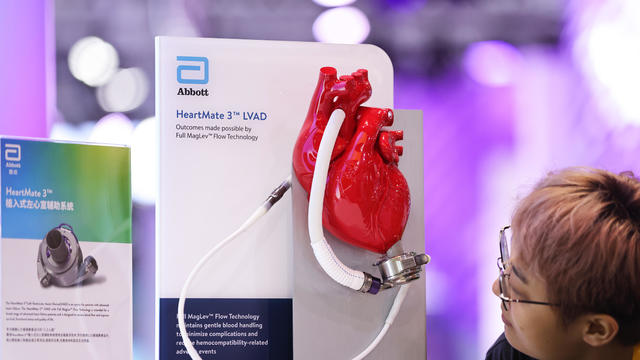
The recall comes years after surgeons say they first noticed problems with the HeartMate II and HeartMate 3, manufactured by Thoratec Corp., a subsidiary of Abbott Laboratories.

Nike's unitard for female track and field athletes representing the U.S. at the 2024 Paris Olympics is too revealing, critics say.

The housing market continues to be challenging for both buyers and sellers this year, as mortgage rates and asking prices continue to climb

The $872 million most likely excludes any amount UnitedHealth may have paid to hackers in ransom.

Bayer has been lobbying lawmakers in three states to pass bills providing it legal protection from suits claiming Roundup causes cancer. Experts say such a measure could have much broader implications.

The price of gold has been up lately, but by how much. Here's how much gold's price has risen since March 1.

There are multiple types of long-term care insurance to choose from. Learn more about cash benefit policies here.

It can be advantageous for homebuyers to pursue these strategies now before the Fed meets again on April 30.

Tesla accounted for 80% of electric vehicle sales in the U.S. in 2020, but that figure fell to 55% last year.
The generative artificial intelligence boom has led to the emergence of romantic companion bots.

Apple said it will stop selling the devices later this month in order to comply with a U.S. import ban.

Alex Jones, the conspiracy theorist known for his fake news site InfoWars and his false denial of the Sandy Hook massacre, was permanently banned from Twitter in 2018.

More than 90 million consumers will scan a QR code this year. But the technology can also facilitate identity theft.
The billionaire owner of X took a defensive tone, saying that "the whole world will know that those advertisers killed the company."

OpenAI co-founder Sam Altman says he's looking forward to returning to the company, with the support of Microsoft's CEO, to build the 2 companies' "strong partnership."

Musk, who is under fire for supporting an antisemitic post, said the money will be donated to hospitals in Israel and to the Red Cross in Gaza.
Altman landed at Microsoft, the biggest investor in OpenAI, as former Twitch leader Emmett Shear was named OpenAI's new chief executive.

Seven Manhattan residents were selected Tuesday afternoon to serve on the jury in former President Donald Trump's criminal trial.

Sen. Bob Menendez heads to trial next month to fight charges that he traded his political influence for cash, gold bars and a luxury car.

The Senate is tasked with the trial after the House impeached Mayorkas earlier this year. Senate Democrats are expected to move to quickly quash the effort.

Trump's allies are encouraging foreign countries to send emissaries to Mar-a-Lago to reconnect ahead of another potential Trump stint in the White House, sources confirmed.

Authorities in Florida said they believe there's a connection between the suspects in the death of a Florida woman and the death of a tow truck driver.

"El Chapo" asked for intervention from the judge in the letter for the "unprecedented discrimination against me."

Both the alleged shooter and the Uber driver appeared to have been targets of scam phone calls, the Clark County Sheriff's Office said.

House Speaker Mike Johnson said Tuesday he won't resign, as another lawmaker calls for him to step down or face an effort to remove him from the top post.
19 people have been stricken — including nine who have been hospitalized — after getting fake or mishandled injections in homes and spas, feds warn.

Former "Monty Python" star Eric Idle said people "always assume we're loaded." He added, "I have to work for my living."

Only about 1 in 10 Americans understands the basics of longevity, or how long they'll live in retirement. Can you pass the test?

Over the next few years, the U.S. could see a surge in seniors living in poverty, one retirement expert predicts.

The gap between what people think they'll need for old age and their actual savings is massive, even for those nearing retirement.

Seniors and other recipients of the Social Security program may get a cost-of-living adjustment of 3.1% next year, one forecast says.

At least 24 states have adopted bans on gender-affirming care for minors in recent years, and most of them face legal challenges.

Viola escaped her circus handler before she was supposed to appear on stage in Butte, Montana.

CBS News Confirmed examines three viral claims that have emerged so far during Trump's first criminal trial.

Veronica Butler and Jillian Kelley's disappearance last month prompted a murder investigation that has led to four arrests.

Strong storms across the central U.S. have caused damage and spawned tornadoes, with more severe storms in the forecast through the night.
Republican governors criticized the UAW's efforts as Volkswagen workers in Tennessee are set to start voting on joining the labor union.
The $872 million most likely excludes any amount UnitedHealth may have paid to hackers in ransom.
The recall comes years after surgeons say they first noticed problems with the HeartMate II and HeartMate 3, manufactured by Thoratec Corp., a subsidiary of Abbott Laboratories.
The former president's media company announced plans to air news, religious channels and other content.
19 people have been stricken — including nine who have been hospitalized — after getting fake or mishandled injections in homes and spas, feds warn.
At least 24 states have adopted bans on gender-affirming care for minors in recent years, and most of them face legal challenges.
CBS News Confirmed examines three viral claims that have emerged so far during Trump's first criminal trial.
Sen. Bob Menendez heads to trial next month to fight charges that he traded his political influence for cash, gold bars and a luxury car.
Trump's allies are encouraging foreign countries to send emissaries to Mar-a-Lago to reconnect ahead of another potential Trump stint in the White House, sources confirmed.
House Speaker Mike Johnson said Tuesday he won't resign, as another lawmaker calls for him to step down or face an effort to remove him from the top post.
The $872 million most likely excludes any amount UnitedHealth may have paid to hackers in ransom.
The recall comes years after surgeons say they first noticed problems with the HeartMate II and HeartMate 3, manufactured by Thoratec Corp., a subsidiary of Abbott Laboratories.
19 people have been stricken — including nine who have been hospitalized — after getting fake or mishandled injections in homes and spas, feds warn.

"Grief has come to us in waves. Moments of feeling absolutely gutted... then moments of feeling blessed by just getting a moment with her," the couple said.

Bella Hadid raised eyebrows after sharing her elaborate morning routine on TikTok, and other over-the-top celebrity self-care rituals are everywhere. Here's what experts suggest you aim for instead.

Normally parched roads and airport runways in the desert city-state of Dubai were left underwater by an incredibly rare rainstorm.
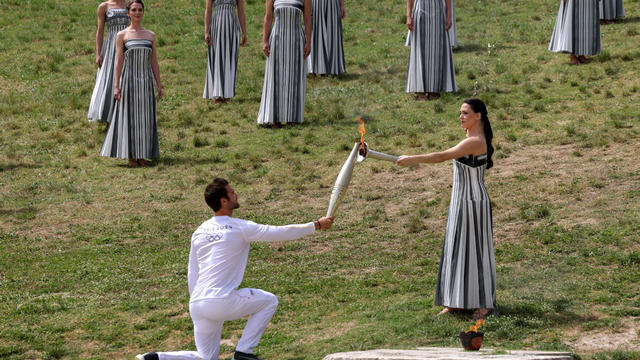
A whopping 10,000 athletes will carry the torch 3,100 miles over 68 days.

A Sudanese-American family is the first to be reunited in the U.S. after a woman and her sons spent nearly a year stuck in Saudi Arabia.

The 17th-century building's iconic spire, thought to protect the building "against enemy attacks and fires," collapsed among the flames.

The House speaker says he wants to put up separate individual bills on aid for Ukraine, Israel, and Taiwan.

ABBA, Blondie and the Notorious B.I.G. were among the 25 artists selected this year to be added to the Library of Congress' National Recording Registry.

Adell remained tight-lipped about her studio time with Beyoncé, urging fans to use their imagination

ABBA, Blondie and The Notorious B.I.G. are entering America's audio canon.
Recognized as one of CMT's "Next Women of Country," Tanner Adell's career soared after her appearances on Beyoncé's latest album. With a 1,500% spike in Spotify listeners and a new single, "Whiskey Blues," Adell is quickly becoming a standout in the country-pop scene.

A Billy Joel special on CBS and Paramount+ will air again after it was cut off in the middle of the singer's performance of "Piano Man."
The former president's media company announced plans to air news, religious channels and other content.
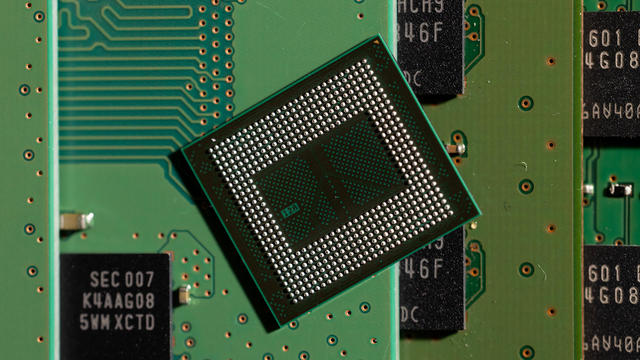
The Biden administration is awarding Samsung $6.4 billion to expand American chipmaking. The company will spread the money across at least five facilities in Texas. Sujai Shivakumar, senior fellow at the Center for Strategic and International Studies, joins CBS News to assess the economic and technological impacts.

From labor shortages to environmental impacts, farmers are looking to AI to help revolutionize the agriculture industry. One California startup, Farm-ng, is tapping into the power of AI and robotics to perform a wide range of tasks, including seeding, weeding and harvesting.

Roku said Friday a second security breach impacted more than 576,000 accounts after announcing in March that 15,000 accounts had been exposed by a hack. Emma Roth, a writer for The Verge, joins CBS News with more details.

The bill reforms and extends a portion of the Foreign Intelligence Surveillance Act known as Section 702 for a shortened period of two years.

A major global coral bleaching event is occurring for the second time in 10 years, according to the National Oceanic and Atmospheric Administration. Derek Manzello, A coral reef ecologist and NOAA reef watch coordinator, joins CBS News with more.
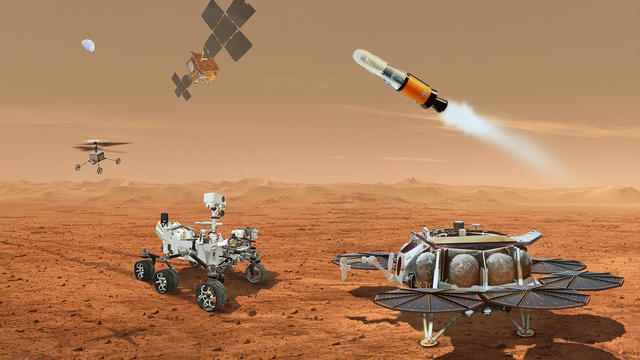
NASA said it agrees with an independent review board that concluded the project could cost up to $11 billion without major changes.

Only 5 to 6% of plastic waste produced in the U.S. is actually recycled. A new report accuses the plastics industry of a decades-long campaign to "mislead" the public about the viability of recycling.

Mexico City, one of the world's most populated cities with nearly 22 million people, could run out of water in months. Florencia Gonzalez Guerra, an investigative video journalist, joins CBS News to examine the causes behind the crisis.

Greenhouse gas emissions continued increasing in 2023, according to new data from the National Oceanic and Atmospheric Administration. CBS News' Elaine Quijano breaks down the numbers and what they mean for the climate.
Veronica Butler and Jillian Kelley's disappearance last month prompted a murder investigation that has led to four arrests.
Both the alleged shooter and the Uber driver appeared to have been targets of scam phone calls, the Clark County Sheriff's Office said.
Authorities in Florida said they believe there's a connection between the suspects in the death of a Florida woman and the death of a tow truck driver.
Seven Manhattan residents were selected Tuesday afternoon to serve on the jury in former President Donald Trump's criminal trial.

A murder trial starts Tuesday for Karen Read, a Massachusetts woman accused of murdering her boyfriend, who was a police officer, in 2022. Her lawyers say Read is being framed as part of a cover up involving multiple law enforcement agencies, and that someone else is responsible.

NASA confirmed Monday that a mystery object that crashed through the roof of a Naples, Florida home last month was space junk from equipment discarded by the space station.
NASA said it agrees with an independent review board that concluded the project could cost up to $11 billion without major changes.

It was a "bittersweet moment" as United Launch Alliance brought the Delta program to a close.

NASA flight engineers managed to photograph and videotape the moon's shadow on Earth about 260 miles below them.

Millions of Americans poured into the solar eclipse’s path of totality to watch in wonder. The excitement was shared across generations for the rare celestial event that saw watch parties across the country as almost all of the continental U.S. saw at least a partial solar eclipse.
A look back at the esteemed personalities who've left us this year, who'd touched us with their innovation, creativity and humanity.

The Francis Scott Key Bridge in Baltimore collapsed early Tuesday, March 26 after a column was struck by a container ship that reportedly lost power, sending vehicles and people into the Patapsco River.

When Tiffiney Crawford was found dead inside her van, authorities believed she might have taken her own life. But could she shoot herself twice in the head with her non-dominant hand?

We look back at the life and career of the longtime host of "Sunday Morning," and "one of the most enduring and most endearing" people in broadcasting.

Cayley Mandadi's mother and stepfather go to extreme lengths to prove her death was no accident.
Viola the elephant was scheduled to perform with the Jordan World Circus in Butte, Montana, before she escaped her handler and took a walk through the city.

The 2024 Olympic torch has been lit ahead of the Summer Games in Paris. CBS News producer Elizabeth Campbell joins with a preview of the event.

Both presidential candidates were in their hometowns for very different reasons Tuesday. CBS News chief White House correspondent Nancy Cordes explains.

Senators will be sworn in as jurors Wednesday in the historic impeachment of Alejandro Mayorkas. CBS News congressional correspondent Scott MacFarlane has the details on how the trial against the Homeland Security secretary is expected to play out.

Supreme Court justices began hearing arguments Tuesday surrounding a key part of the Jan. 6 prosecutions. The case revolves around the use of a federal obstruction statute. CBS News legal contributor Jessica Levinson joins to break it all down.