
TikTok ban measure passed by the Senate. Here's what could happen next.
Senators approve foreign aid package that includes a potential ban on TikTok in the U.S. Here's what experts say could happen next.
Watch CBS News
Senators approve foreign aid package that includes a potential ban on TikTok in the U.S. Here's what experts say could happen next.

Regulators prohibit new noncompetes, which impede millions of U.S. workers from getting a better job.

Former President Donald Trump could receive a large windfall from his newly public media company, Trump Media & Technology Group.

Tesla reports slide in earnings and revenue, but investors cheered by pledge to accelerate rollout of cheaper vehicles.

Customers who rely on government assistance programs can get same perks as Prime members, for less.

UnitedHealth said it paid the criminals behind attack that crippled hospitals and pharmacies to protect sensitive patient data.

A "concierge service" that lets paying members bypass airport security lines is unfair to other travelers, California lawmaker says.

Millions of Americans filed their taxes during the last two weeks of this year's tax season. Here's how to find out when you'll get your refund.

Travelers often spend more than they need to for airfare, experts say. Here's what to know about paying for add-ons like your seat assignment.

How much money can you save by paying off $20,000 in credit card debt with your home equity? Find out now.

A mortgage loan denial is disheartening, but there are ways to improve your chances of future approval.

If you're looking for ways to resolve your overwhelming credit card debt, these strategies are worth considering.

Tesla accounted for 80% of electric vehicle sales in the U.S. in 2020, but that figure fell to 55% last year.
The generative artificial intelligence boom has led to the emergence of romantic companion bots.

Apple said it will stop selling the devices later this month in order to comply with a U.S. import ban.

Alex Jones, the conspiracy theorist known for his fake news site InfoWars and his false denial of the Sandy Hook massacre, was permanently banned from Twitter in 2018.

More than 90 million consumers will scan a QR code this year. But the technology can also facilitate identity theft.
The billionaire owner of X took a defensive tone, saying that "the whole world will know that those advertisers killed the company."

OpenAI co-founder Sam Altman says he's looking forward to returning to the company, with the support of Microsoft's CEO, to build the 2 companies' "strong partnership."

Musk, who is under fire for supporting an antisemitic post, said the money will be donated to hospitals in Israel and to the Red Cross in Gaza.
Altman landed at Microsoft, the biggest investor in OpenAI, as former Twitch leader Emmett Shear was named OpenAI's new chief executive.

After months of disagreement in Congress, the Senate approved the package and sent it to President Biden. It includes a provision that could lead to a ban of TikTok.

Jurors in Donald Trump's trial in New York heard testimony from a former media executive about his efforts to bury negative stories about Trump before the 2016 presidential election.
Senators approve foreign aid package that includes a potential ban on TikTok in the U.S. Here's what experts say could happen next.

The school had set a deadline of midnight Wednesday for it to reach an agreement with demonstrators about dispersing their encampment but extended that deadline early Wednesday for 48 hours.

It comes over a year after a shooting at a Nashville school killed three children and three adults.

Former New York Rep. George Santos is no longer running for Congress, he announced Tuesday on X.

Earlier this month, the Arizona Supreme Court ruled that the highly-restrictive 160-year-old law that bans nearly all abortions can be enforced.

The former officer, Elias Huizar, is suspected of killing two women and abducting a child in central Washington.

Larry Webb confessed to shooting and killing Susan and Natasha "Alex" Carter, who had been missing for 24 years, officials said.

The U.S. is reaching "peak 65," marking the largest retirement wave in American history. But the financial outlook for many is grim.

Americans are underprepared for retirement, with the average account holding just $88,400 in savings.
BlackRock CEO Larry Fink said that longer life expectancies are "putting the U.S. retirement system under immense strain."

About 1 in 8 workers think they'll retire by age 61. But the reality of saving for decades of expenses is daunting.

America's retirement system has left behind 90% of workers. "We see big gaps with the rich and the poor in terms of who gets to retire," one expert said.
Travelers often spend more than they need to for airfare, experts say. Here's what to know about paying for add-ons like your seat assignment.
Earlier this month, the Arizona Supreme Court ruled that the highly-restrictive 160-year-old law that bans nearly all abortions can be enforced.
It comes over a year after a shooting at a Nashville school killed three children and three adults.
Jurors in former President Donald Trump's trial in New York heard testimony from a former media executive about his efforts to bury negative stories about Trump before the 2016 presidential election.

Ryan Watson could face at least 12 years in prison in Turks and Caicos after airport security allegedly found four rounds of hunting ammo in his carry-on.
Travelers often spend more than they need to for airfare, experts say. Here's what to know about paying for add-ons like your seat assignment.
Tesla reports slide in earnings and revenue, but investors cheered by pledge to accelerate rollout of cheaper vehicles.
Regulators prohibit new noncompetes, which impede millions of U.S. workers from getting a better job.
Customers who rely on government assistance programs can get same perks as Prime members, for less.
UnitedHealth said it paid the criminals behind attack that crippled hospitals and pharmacies to protect sensitive patient data.
Earlier this month, the Arizona Supreme Court ruled that the highly-restrictive 160-year-old law that bans nearly all abortions can be enforced.
It comes over a year after a shooting at a Nashville school killed three children and three adults.
Jurors in former President Donald Trump's trial in New York heard testimony from a former media executive about his efforts to bury negative stories about Trump before the 2016 presidential election.
"He's ultimately responsible," former House Speaker Nancy Pelosi said of Israeli Prime Minister Benjamin Netanyahu.
Former New York Rep. George Santos is no longer running for Congress, he announced Tuesday on X.
UnitedHealth said it paid the criminals behind attack that crippled hospitals and pharmacies to protect sensitive patient data.
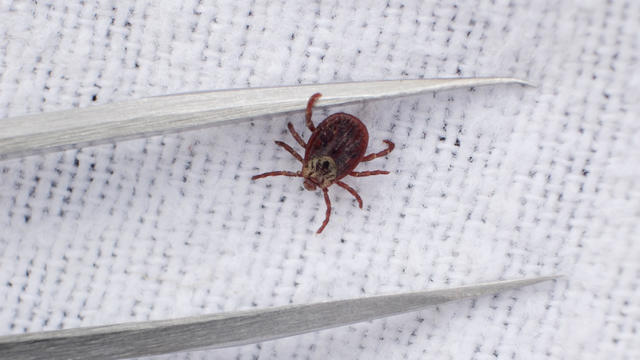
Warmer weather is prime time for ticks that can carry Lyme disease and other illnesses. Here's how to spot them and get rid of them.

Tires emit huge volumes of particles and chemicals as they roll along the highway, and researchers are only beginning to understand the threat. One byproduct of tire use, 6PPD-q, is in regulators' crosshairs after it was found to be killing fish.

Cancer, heart disease, respiratory illnesses and kidney dysfunction among the health consequences of a warming planet.
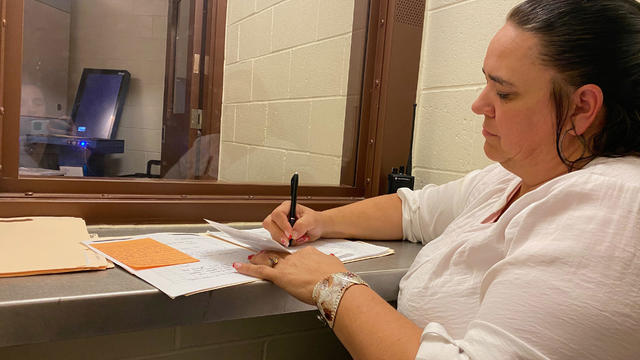
To reduce recidivism, some rural counties are hiring community health workers or peer support specialists to connect people leaving custody to mental health, substance use treatment, medical services and jobs.
Ryan Watson could face at least 12 years in prison in Turks and Caicos after airport security allegedly found four rounds of hunting ammo in his carry-on.

This will be the first General Conference since more than 7,600 mostly conservative congregations left the United Methodist Church between 2019 and 2023.
Columbia University has extended the deadline to reach an agreement with pro-Palestinian demonstrators about dispersing their encampment.
"He's ultimately responsible," former House Speaker Nancy Pelosi said of Israeli Prime Minister Benjamin Netanyahu.

Six men have been arrested on suspicion of involvement in the drug's transport, a Swedish customs official said.

Surprise guests, a broken foot and a history-making headliner.

Eric Church is revered as one of country music's most respected figures, often described as Nashville's renegade. But he admits that even after his success, he sometimes still sees himself as an outsider.
Angel Carter Conrad talks about her brother Aaron Carter, his death and how she hopes his legacy and previously unheard music can help others.

Emmy and Tony Award-winning actress Bebe Neuwirth is back on Broadway, starring as Fraulein Schneider in the new revival of "Cabaret."

Chanel Miller, celebrated for her profound memoir "Know My Name," steps into a new creative realm with her children's book "Magnolia Wu Unfolds It All." The story, both written and illustrated by Miller, follows two young friends on an adventurous quest through New York City to return misplaced socks from Magnolia's parents' laundromat.

NASA's Voyager 1, the first spacecraft to travel beyond our solar system, has started sending information back to Earth again after scientists managed to fix the probe from 15 billion miles away.
Customers who rely on government assistance programs can get same perks as Prime members, for less.

From labor shortages to environmental impacts, farmers are looking to AI to help revolutionize the agriculture industry. One California startup, Farm-ng, is tapping into the power of AI and robotics to perform a wide range of tasks, including seeding, weeding and harvesting.

Secretary of Commerce Gina Raimondo is at the center of a global competition for semiconductor dominance. It's a battle that also puts her at the center of two of the hottest global national security hotspots. Lesley Stahl of 60 Minutes spoke with Raimondo for the broadcast.
Senators approve foreign aid package that includes a potential ban on TikTok in the U.S. Here's what experts say could happen next.

The White House is considering declaring a national climate emergency to unlock federal powers and stifle oil development, according to a Bloomberg report. Meanwhile, the Biden administration is announcing several projects this Earth Week. Columbia University Climate School professor Dr. Melissa Lott joins with analysis.
NASA's Voyager 1, the first spacecraft to travel beyond our solar system, has started sending information back to Earth again after scientists managed to fix the probe from 15 billion miles away.
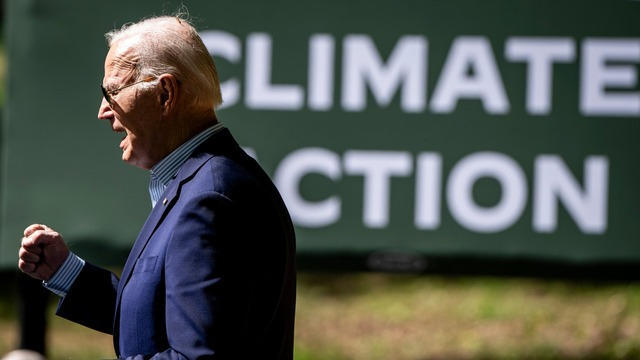
Relatively few Americans say they know a lot about President Biden's initiatives to combat climate change, according to a CBS News poll. Carolyn Kissane, a New York University global affairs associate dean and professor, joins CBS News with more on Biden's climate policies.
A photo taken two days after the sinking of the RMS Titanic apparently shows the iceberg that doomed the so-called unsinkable ship in 1912. CBS News' John Dickerson has details.

Despite how terrifying sharks might seem, the creatures are critical to the survival of the world's oceans. Oceans generate 50% of the oxygen on the planet and absorb 90% of excess heat created by global warming. CBS News senior national and environmental correspondent Ben Tracy spoke with conservationists in the Bahamas.

CBS News is investigating a growing number of fraud cases known as romance scams. Chief investigative correspondent Jim Axelrod explains how victims can unknowingly become perpetrators in the very scams they fall prey to.

Jim Axelrod dives into the world of romance scams, showing how sometimes the victims can also become unwitting accomplices in the scammers' financial crimes.

Don Steven McDougal, a family friend, was indicted by a Polk County grand jury in connection with the death of an 11-year-old girl.
Six men have been arrested on suspicion of involvement in the drug's transport, a Swedish customs official said.
Larry Webb confessed to shooting and killing Susan and Natasha "Alex" Carter, who had been missing for 24 years, officials said.

In November 2023, NASA's Voyager 1 spacecraft stopped sending "readable science and engineering data."

In two weeks, Boeing's Starliner spacecraft is scheduled to launch its first piloted test flight, bringing two veteran NASA astronauts to the International Space Station. Astronaut Matt Dominick joined CBS News from the ISS to talk about the mission and life in space.

A process called cryopreservation allows cells to remain frozen but alive for hundreds of years. For some animal cells, the moon is the closest place that's cold enough.

The Lyrid meteor show is set to peak as the week begins.

April's full moon, known as the Pink Moon, will reach peak illumination on Tuesday, but it will appear full from Monday morning through Thursday morning.
A look back at the esteemed personalities who've left us this year, who'd touched us with their innovation, creativity and humanity.

The Francis Scott Key Bridge in Baltimore collapsed early Tuesday, March 26 after a column was struck by a container ship that reportedly lost power, sending vehicles and people into the Patapsco River.

When Tiffiney Crawford was found dead inside her van, authorities believed she might have taken her own life. But could she shoot herself twice in the head with her non-dominant hand?

We look back at the life and career of the longtime host of "Sunday Morning," and "one of the most enduring and most endearing" people in broadcasting.

Cayley Mandadi's mother and stepfather go to extreme lengths to prove her death was no accident.

Seventeen-year-old Gukesh Dommaraju of India is the youngest challenger for the world chess title later this year. CBS News' John Dickerson has the details.
CBS News is investigating a growing number of fraud cases known as romance scams. Chief investigative correspondent Jim Axelrod explains how victims can unknowingly become perpetrators in the very scams they fall prey to.
The White House is considering declaring a national climate emergency to unlock federal powers and stifle oil development, according to a Bloomberg report. Meanwhile, the Biden administration is announcing several projects this Earth Week. Columbia University Climate School professor Dr. Melissa Lott joins with analysis.

Teachers are in short supply in the U.S., and researchers say there's declining job satisfaction among those who remain. CBS News reporter Bo Erickson examines what's behind the problems.

The U.S. is close to delivering a $61 billion aid package to the Ukrainian military, and Russia's defense minister said Tuesday that Moscow would ramp up its own weapons production in response. William Taylor, former U.S. ambassador to Ukraine, joins CBS News to discuss.